- Компании
- Takeda. О компании, буклеты, каталоги, контакты
- Olympus. О компании, буклеты, каталоги, контакты
- Boston Scientific. О компании, буклеты, каталоги, контакты
- Pentax. О компании, буклеты, каталоги, контакты
- Fujifilm & R-Farm. О компании, буклеты, каталоги, контакты
- Erbe. О компании, буклеты, каталоги, контакты
- Еще каталоги
- Мероприятия
- Информация
- Обучение
- Классификации
- Атлас
- Quiz
- Разделы
- Пациенту







")







 клинические рекомендации 2024")
QR-код этой страницы
Для продолжения изучения на мобильном устройстве ПРОСКАНИРУЙТЕ QR-код с помощью спец. программы или фотокамеры мобильного устройства
Случайный выбор
данная функция, случайным образом выбирает информацию для Вашего изучения,
запустите выбор нажав кнопку ниже
Обратная связь
Напишите нам
Статьи: Z-линия пищевода. Классификация зубчатой линии ZAP. Endoscopic assessment of the “Z-line” (squamocolumnar junction) appearance: reproducibility of the ZAP classification among endoscopists
| Авторы: | |
| Об авторах: |
1. Uppsala University Hospital 2. Uppsala University Hospital |
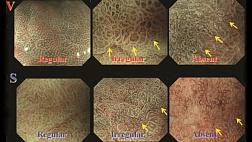
Классификация ZAP для определения внешнего вида Z-линии выглядит следующим образом:
• Grade 0: Z-линия острая и круглая. Линия может быть волнообразной из-за складок слизистой, но без узких линейных расширений (язычков) или столбчатых островков• 1 степени: Z-линия нерегулярна и cуществуют похожие на язык выступы и / или островки столбчатого эпителия.
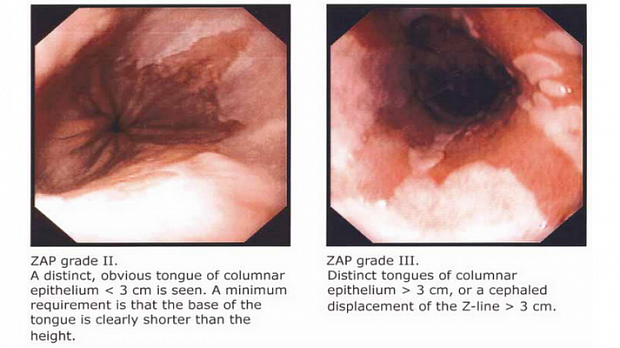
• II степени: отчетливый, очевидный язык столбчато-появляется эпителия меньше 3 см в длину присутствует. Минимальное требование состоит в том, что ширина у основания языка должна быть меньше его длины.
• III степени: присутствуют отчетливые языки столбчатого эпителия длиной более 3 см или наблюдается смещение цефалад Z-линии более 3 см.
Аннотация:
Отделение хирургических наук, Упсальская университетская больница, Упсала, Швеция.
Фон : гистологическое присутствие кишечной метаплазии в пищеводе является необходимым условием для диагностики пищевода Барретта. Таким образом, использование термина пищевода Барретта для описания определенных эндоскопических особенностей дистального отдела пищевода нецелесообразно. Не существует общепринятой системы классификации для эндоскопического описания плоскоклеточного слизистого перехода, так называемой «Z-линии». Кроме того, не существует четкого определения нормальной Z-линии. Предложена классификация внешнего вида Z-линии: классификация ZAP. Целью данного исследования было оценить воспроизводимость этой классификации.
Методы: Десять врачей с различным опытом эндоскопии получили 15 эндоскопических фотографий Z-линии, и им было предложено классифицировать их в соответствии с классификацией ZAP. Вторая оценка была проведена между 7 и 15 неделями после первой.
Результаты: Медианные значения каппа находились в диапазоне от 0,72 до 0,90 в отношении внутриобозревательной, а также воспроизводимости между наблюдателями, независимо от опыта с верхней эндоскопией.
Выводы: внутриобозревательная и межобозревательная воспроизводимость классификации ZAP является существенной, и, таким образом, целесообразно использовать эту классификацию для характеристики появления Z-линии при эндоскопии.
Abstract
Background: The histologic presence of intestinal metaplasia in the esophagus is a prerequisite for the diagnosis of Barrett's esophagus. Thus, use of the term Barrett's esophagus to describe certain endoscopic features in the distal esophagus is inappropriate. There is no accepted classification system for the endoscopic description of the squamocolumnar mucosal junction, the so-called “Z-line.” Furthermore, no clear definition of the normal Z-line exists. A classification of the Z-line appearance has been proposed: the ZAP classification. The aim of this study was to assess the reproducibility of this classification.
Methods: Ten physicians with varying endoscopy experience were presented with 15 endoscopic photographs of the Z-line and were asked to classify them according to the ZAP classification. A second assessment was conducted between 7 and 15 weeks after the first. Results: The median κ values were in the range of 0.72 to 0.90 with regard to intraobserver as well as interobserver reproducibility, irrespective of experience with upper endoscopy.
Conclusions: The intraobserver and interobserver reproducibility of the ZAP classification is substantial and thus it is feasible to use this classification to characterize the appearance of the Z-line at endoscopy. ( GASTROINTESTINAL ENDOSCOPY 2002;55:65-9.)
 appearance Reproducibility.png)
 - Adobe Acrobat Pro DC.png)
 - Adobe Acrobat Pro DC.png)
 - Adobe Acrobat Pro DC.png)
 - Adobe Acrobat Pro DC.png)
 - Adobe Acrobat Pro DC.png)
 - Adobe Acrobat Pro DC.png)
 appearance Reproducibility.png)
 - Adobe Acrobat Pro DC.png)
 - Adobe Acrobat Pro DC.png)
 - Adobe Acrobat Pro DC.png)
 - Adobe Acrobat Pro DC.png)
 - Adobe Acrobat Pro DC.png)
 - Adobe Acrobat Pro DC.png)
Полный текст статьи:
The ZAP classification of the appearance of the Z-line isas follows:
- Grade 0: The Z-line is sharp and circular. The Zline may be wave-like because of the mucosal folds, but no narrow linear extensions (tongues) or islands of columnarepithelium are present.
- Grade I: The Z-line is irregular and there are tongue-like protrusions and/or islands of columnar-appearing epithelium.
- Grade II: A distinct, obvious tongue of columnar-appearing epithelium less than 3 cm in length is present. A minimum requirement is that the width at the base of the tongue must be less than its length.
- Grade III: Distinct tongues of columnar-appearing epithelium greater than 3 cm in length are present, or there is a cephalad displacement of the Z-line more than 3 cm.
Полный текст доступен пользователям с подпиской

Классификация ZAP, вероятно, будет интересна для практического и повсеместного применения в России, однако до принятия ее Эндоскопическим сообществом может пройти очень много времени.
Вывод:
внутриобозревательная и межобозревательная воспроизводимость классификации ZAP является существенной, и, таким образом, целесообразно использовать эту классификацию для характеристики появления Z-линии при эндоскопии. ( GASTROINTESTINAL ENDOSCOPY 2002; 55: 65-9.)
Список литературы:
От редакции EndoExpert.ru
#Классификации
Рекомендуемые статьи
.jpg)


.png)
Эндоскопическая ретроградная холангиопанкреатография
- рентген-эндоскопический метод диагностики патологии желчных и панкреатических протоков.
При эндоскопическом исследовании в случае бронхоэктазов в стадии ремиссии выявляется
частично диффузный бронхит I степени воспаления
.jpg)

Присоединяйтесь к нам в социальных сетях





Работаем и учимся при поддержке


Партнеры


Добро пожаловать на информационно-образовательный
медицинский портал EndoExpert.ru
Вы находитесь в разделе предназначенном только для специалистов (раздел для пациентов по ссылке). Пожалуйста, внимательно прочитайте полные условия использования и подтвердите, что Вы являетесь медицинским или фармацевтическим работником или студентом медицинского образовательного учреждения и подтверждаете своё понимание и согласие с тем, что применение рецептурных препаратов, обращение за той или иной медицинской услугой, равно как и ее выполнение, использование медицинских изделий, выбор метода профилактики, диагностики, лечения, медицинской реабилитации, равно как и их применение, возможны только после предварительной консультации со специалистом. Мы используем файлы cookie, чтобы предложить Вам лучший опыт взаимодействия. Файлы cookie позволяют адаптировать веб-сайты к вашим интересам и предпочтениям.
Я прочитал и настоящим принимаю вышеизложенное, хочу продолжить ознакомление с размещенной на данном сайте информацией для специалистов.
Комментарии